The main total hysterectomy ICD 10 status code is Z90.710, which means acquired absence of both the uterus and cervix. It is generally used in medical records after a patient has undergone a total hysterectomy.
This code describes the person’s current anatomy. It does not show why the operation was performed, how the surgery was completed, whether the ovaries were removed, or whether complications occurred. Those details may require separate codes and supporting documentation.
What Does a Total Hysterectomy Remove?
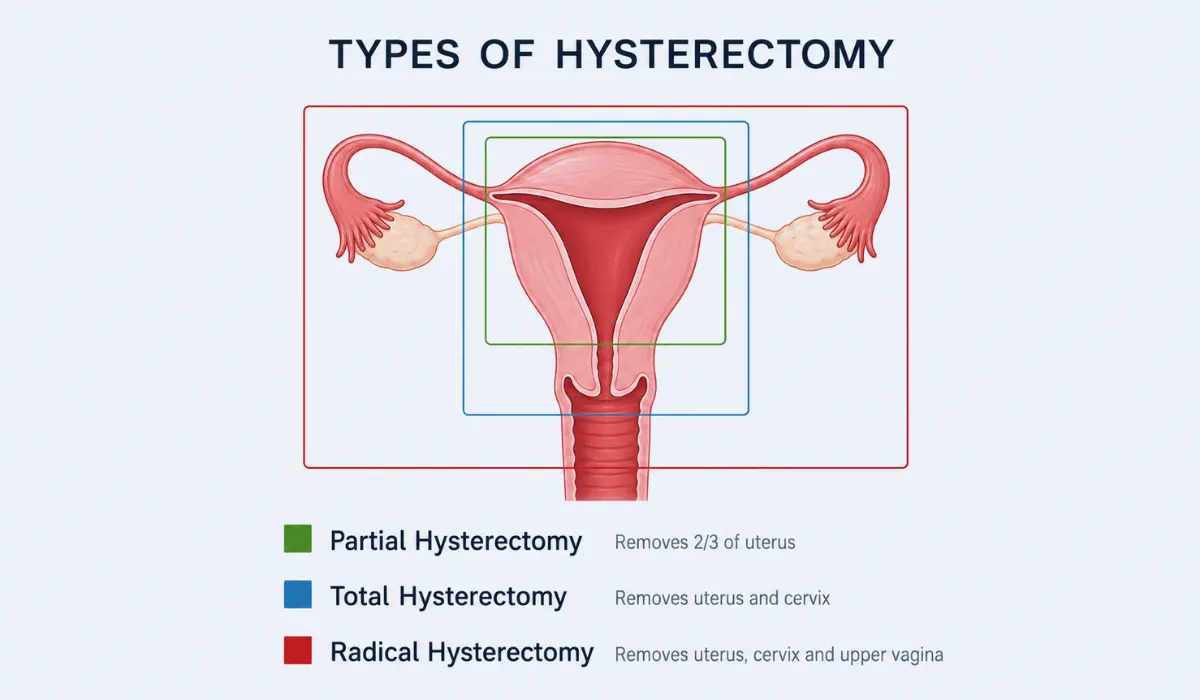
A total hysterectomy removes the uterus and cervix. It may be performed through the abdomen, vagina, or with laparoscopic or robotic techniques. Many people ask whether a hysterectomy stops periods. Once the uterus is removed, menstrual bleeding ends permanently.
Despite the word “total,” this procedure does not automatically include the ovaries. The fallopian tubes or ovaries may be removed during the same operation, but these are separate surgical decisions.
After removal of the uterus, menstrual periods stop and pregnancy can no longer be carried. Whether menopause begins immediately depends mainly on whether both ovaries were also removed.
What Is the Correct ICD-10 Code?
Z90.710: Acquired Absence of Both Cervix and Uterus
For FY 2026, Z90.710 is the specific ICD-10-CM code associated with acquired absence of both the cervix and uterus. Its inclusion terms cover status after a total hysterectomy.
The broader category Z90.71 refers to acquired absence of the cervix and uterus, but it is a parent category. A more detailed code, such as Z90.710, should be selected when the documentation supports it.
ICD-10-CM code sets are updated regularly. Healthcare professionals should verify the version that applies to the date of service rather than relying on an old claim or website.
How Is It Different From the Partial Hysterectomy Code?
A partial, subtotal, or supracervical hysterectomy removes the main part of the uterus but leaves the cervix in place. This status is represented by:
- Z90.711: Acquired absence of uterus with remaining cervical stump
The distinction matters because someone with a remaining cervix may still need cervical cancer screening based on age, health history, and previous test results.
A partial hysterectomy removes the uterus while leaving the cervix in place, so it uses a different ICD-10-CM status code from a total hysterectomy.
Another related code is Z90.712, which means the cervix is absent while the uterus remains. This is different from both total and partial hysterectomy status.
Does Z90.710 Include Ovary Removal?
No. Z90.710 only describes the absence of the uterus and cervix. When one or both ovaries were removed, another status code may also be appropriate:
- Z90.721: Acquired absence of one ovary
- Z90.722: Acquired absence of both ovaries
- Z90.79: Acquired absence of another genital organ, which may apply to removed fallopian tubes
The correct combination depends on the operative report and the reason for the medical encounter.
Removing both ovaries can cause surgical menopause in someone who has not already reached menopause. Keeping the ovaries usually allows hormone production to continue until ovarian function declines naturally.
Status Code Versus Procedure Code
Z90.710 is an ICD-10-CM diagnosis or health-status code. It records that the uterus and cervix are no longer present. It is not the code used to describe every technical detail of the original operation.
ICD-10-PCS is used to report inpatient hospital procedures. Other procedure coding systems may apply in outpatient or professional billing. The operative route, organs removed, surgical approach, and reason for surgery influence procedure-code selection.
For example, two patients may both have Z90.710 in their records even though one underwent an abdominal hysterectomy for fibroids and the other had robotic surgery for uterine cancer.
Why Accurate Documentation Matters?
Doctors and coders should confirm whether the cervix, uterus, ovaries, and fallopian tubes were removed. Phrases such as “history of hysterectomy” may not provide enough detail to choose the most specific code.
Useful documents include:
- Operative reports
- Hospital discharge summaries
- Pathology reports
- Gynecology notes
- Cancer treatment summaries
The official coding guidelines emphasize complete and consistent medical documentation. When the anatomy or reason for surgery is unclear, the provider may need to clarify the record before coding is completed.
Practical Health and Record-Keeping Tips
Keep a copy of your hysterectomy operative report and note whether your cervix and ovaries remain. This information can guide future cervical screening, menopause care, imaging interpretation, and evaluation of pelvic symptoms. People with persistent pelvic pain may also need evaluation for endometriosis after hysterectomy, since lesions outside the uterus can remain or cause symptoms later.
Continue routine gynecological care even after a total hysterectomy. Cervical screening may no longer be needed after removal of the cervix for a noncancerous condition, but different guidance can apply after cervical precancer or cancer.
Contact the medical office if your records list a partial hysterectomy when both the uterus and cervix were removed, or if an insurance statement contains a code you do not understand.
When to Seek Professional Help?
Speak with a gynecologist about new vaginal bleeding, persistent pelvic or abdominal pain, unusual discharge, painful urination, or symptoms that interfere with daily life.
After recent surgery, contact the surgical team for worsening pain, fever, vomiting, wound redness, difficulty urinating, or bleeding heavier than a menstrual period. Severe bleeding, fainting, breathing difficulty, or sudden intense pain requires urgent care.
Final Thoughts
The most specific total hysterectomy ICD-10-CM code is Z90.710, which identifies acquired absence of both the uterus and cervix. Z90.711 is used when the uterus was removed but the cervix remains.
The code does not automatically include removal of the ovaries or explain the original reason for surgery. Accurate coding depends on the operative report, current medical circumstances, and the code set in effect on the date of care.
FAQs
Z90.710 is the ICD-10-CM status code for acquired absence of both the uterus and cervix, which generally describes a completed total hysterectomy in medical records and insurance claims.
Z90.711 applies when the uterus was removed but the cervical stump remains. This usually reflects a supracervical, subtotal, or partial hysterectomy rather than a total hysterectomy.
No. Total hysterectomy describes removal of the uterus and cervix. Ovarian removal is separate and may require Z90.721 or Z90.722 as an additional status code when documented.
Not by itself. Z90.710 records the current anatomical status. The reason for surgery, active conditions, complications, and cancer history may need separate codes based on documentation.
ICD-10-CM records diagnoses and health status. The surgery itself may be represented by ICD-10-PCS for inpatient care or another procedure coding system, depending on care setting.
Contact your gynecologist for new bleeding, persistent pelvic pain, unusual discharge, fever, or urinary problems. Heavy bleeding, fainting, or severe pain needs urgent care immediately.